








Image via Wikimedia Commons
Hernia
The word hernia has its origin from the Greek word ‘hernios’ which basically means a protrusion, a bud, or shoot.
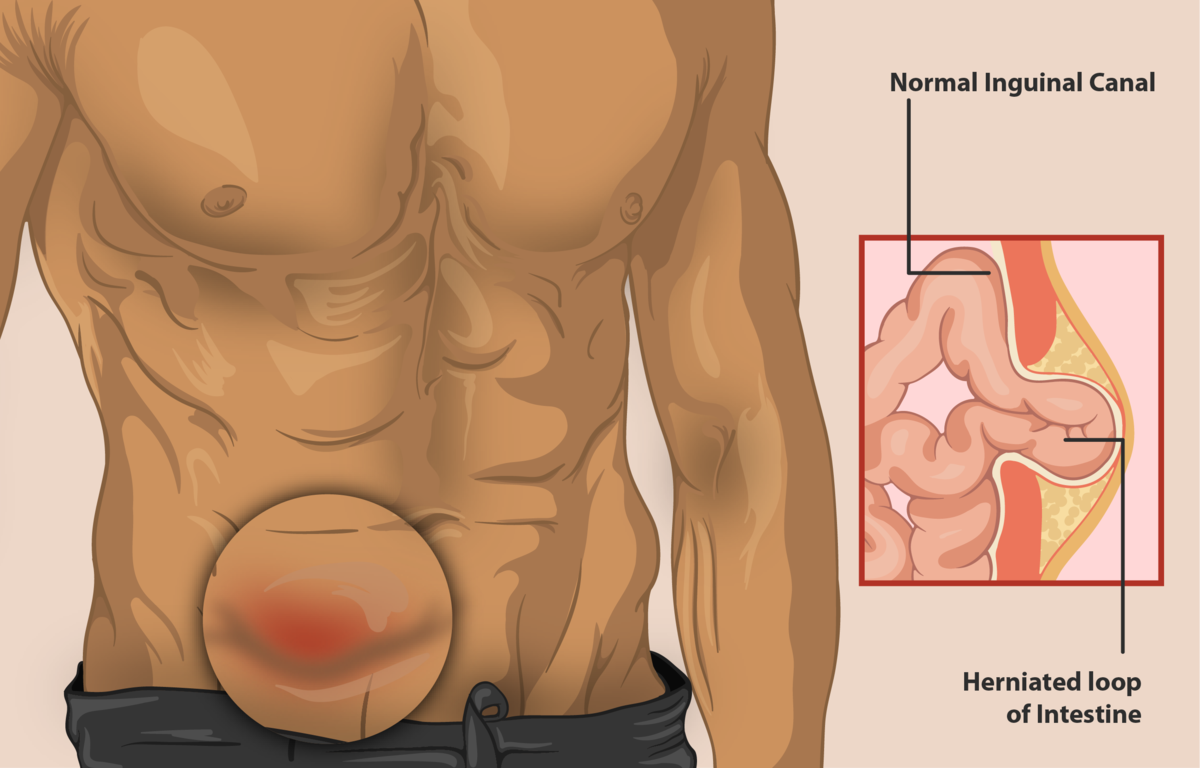
A hernia may be defined as a protrusion of an organ or part of an organ projecting through an opening in its walls.
It is formed when an internal part of the body pushes through a weakness in the muscle or surrounding tissue wall.
A common sign of a hernia is a clear bulge under the skin in the groin or abdomen region. It can cause pain when you lift anything heavy, cough, or strain your body.
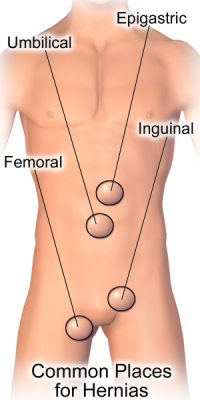
Although it occurs commonly in the abdomen, it may also occur in other regions of the body such as the thorax and cranium.
The lump can sometimes be flattered or be pushed back by lying down. Hernia in this stage is known as reducible hernia and is not considered an emergency, although medical consultation is necessary.
Sometimes the blood supply to the herniated tissue is cut off causing strangulation. This is referred to as a strangulated hernia causing severe pain.
A strangulated hernia may require emergency surgery. A strangulated hernia can occur at any stage in a person’s life and is found in infants, children, and adults.
When the herniated tissue gets trapped and cannot be pushed back, and the blood supply is not cut off, it is called an incarcerated hernia.
Incarcerated hernias, can lead to strangulated hernias. Pain should be considered a very serious warning as those that hurt are more likely to strangulate.
Overexertion, obesity, incorrect weight lifting, chronic constipation, poor nutrition, and several other conditions can cause a hernia.
Diagnosis of Hernia
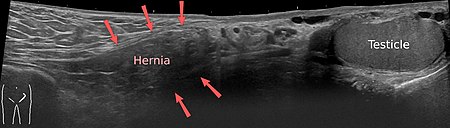
Häggström, M (2014). “Medical gallery of Mikael Häggström 2014 (Ultrasound of Hernia)
A diagnosis of hernia can be made by a physical examination, assessment of symptoms, and an ultrasound scan.
Doctors may also use other imaging techniques such as computed tomography (CT scan) or magnetic resonance imaging (MRI) to study a hernia.
Surgery for Hernia
After a diagnosis has been confirmed, the doctor will determine whether surgery to repair the hernia is necessary depending on the age of the patient, type of hernia, how serious the symptoms are, and other underlying medical conditions.
Although most hernias will not get better without surgery, they will not necessarily get worse when left untreated.
However is some cases, surgery may be the only option when they are strangulated or are at risk of getting strangulated leading to bowel obstruction.
In some cases, the risks of surgery outweigh the potential benefits and the doctor takes the right decision depending on the general health status of the patient.
There are two surgical techniques used in hernia repair both of which utilize a piece of synthetic, or prosthetic, mesh to strengthen the weakness in the abdominal wall.
Surgery may not be best for patients who have had previous surgeries such as abdominal surgery or prostate surgery.
Open hernia repair surgery
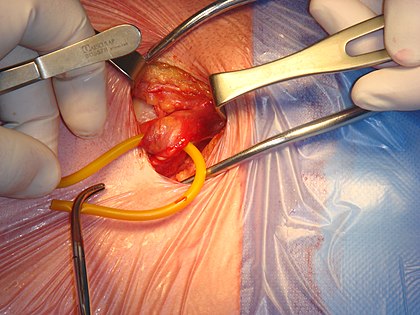
Open surgical repair of a right inguinal hernia. Image: Wikipedia
Usually done to repair small hernias, the surgeon makes a 3-4 inch single long incision directly over the hernia to get to the defect.
The surgeon then takes a call on whether to gently push the hernia back into place, tie it off, or remove it.
The surgeon may choose to sew the prosthetic mesh to the abdominal wall to repair the defect.
This procedure is done on an outpatient basis, often under local anesthesia.
Local anesthesia is a medicine used to numb a particular part of the body.
Hernia repair using Laparoscopic Surgery (Keyhole Surgery)
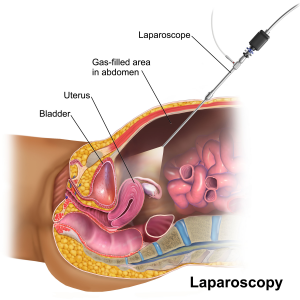
Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”
In this procedure, the hernia may be repaired using a laparoscope (a tiny lighted telescope) connected to a special camera to view the hernia on a video screen. This is performed while the patient is under general anesthesia.
The surgeon inserts instruments to repair the hernia by making several other small incisions in the lower abdominal wall at some distance from the hernia defect.
In this procedure, the hernia is repaired from behind the abdominal wall.
Carbon dioxide gas is used to inflate the abdominal cavity as it gives a better view of the organs and also gives the surgeon space to work inside the patient.
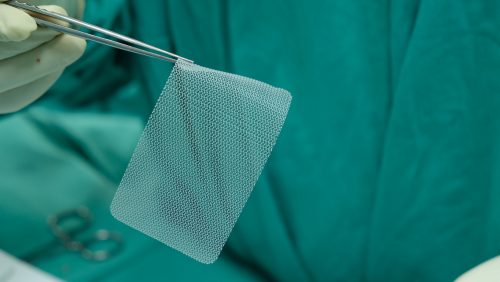
During hernia surgery, surgeons may use a piece of mesh to close and strengthen the abdominal wall. Image Credit: NHS
A small mesh prosthesis is then passed through one of the tubes into the abdomen and fixed to the undersurface of the abdominal wall with stitches and staples.
This technique is used for both small and large hernias of the abdomen. Patients recover from laparoscopic hernia repair surgery within 1-2 weeks.
Patients prefer laparoscopy over open surgical repair as there are smaller incisions and repair of a recurrent hernia is easier using this procedure.
Complications after hernia surgery
Hernia repair is one of the most common surgical procedures performed in the world today and is generally considered safe. As with all surgeries, there is a small risk of complications occurring after surgery. They are:
- Recurrence of Hernia
- Infection
- Long term pain in the scrotum
- Bleeding, drainage, or redness in the surgery area
- Bladder Injury
- Rejection of mesh
- Allergic reaction to anesthesia
- Injury to the intestine and other organs
- Constipation
- Nerve damage
Factors that may increase your risk of developing complications:
- Older age (over 50 years)
- Having a femoral or scrotal hernia
- The hernia has been present for under one year
- Obesity
- Heart disease
Types of hernia
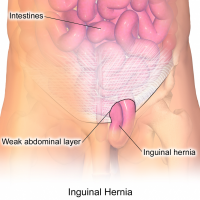
Inguinal hernias (also called groin hernias)
Inguinal hernias are the most common and occur when fatty tissue or a part of your intestine protrudes into the groin area through the defect in the abdominal wall, creating a bulge on the right or left side at the top of your inner thigh.
Credit: Bruce Blaus
They occur through the inguinal canal (conduit where the testicle comes through on its way to the scrotum during the development of males) and are the most common type of hernia in men.
It’s often associated with aging, physical exertion, and strain. It often gets worse throughout the day and improves when lying down
There are two types of Inguinal Hernias-Direct Inguinal Hernia and Indirect Inguinal Hernia.
An indirect inguinal hernia is the most common type of hernia and occurs mostly in males.
Common in children it occurs when tissue protrudes through a vulnerable/weak point in the abdominal muscles.
It is the result of a congenital defect in the lower abdominal wall.
Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014” Wikimedia Commons
In a developing fetus, the inguinal canals have openings inside the abdomen that typically close before birth.
In some cases, one or both openings remain open.
Contents of the abdomen may bulge through this opening, causing a hernia.
Indirect inguinal hernias are more likely to cause bowel obstruction compared to direct inguinal hernias as the inguinal canal can be narrow.
Direct hernias are acquired rather than congenital and are rare in women and children.
They often occur in people aged 25 or older. This hernia occurs due to progressive weakening of the abdominal wall muscles. Contents of the abdomen may bulge out through this weak area, causing a hernia.
Femoral hernias
Femoral hernias are less common accounting for only 3% of all hernias and also happen when fatty tissue or part of your bowel protrudes into the groin area at the top of your inner thigh.
They are less common than inguinal hernias and tend to affect more women than men.
Femoral hernias are also associated with aging, physical exertion, and strain.
Umbilical hernias

Milliways, CC BY-SA 3.0 Wikimedia Commons
Umbilical hernias occur when fatty tissue or part of your bowel pokes through your tummy near your navel causing the belly button to bulge.
This type of hernia can occur in babies if the opening in the tummy that the umbilical cord passes through does not close properly after birth.
This type of hernia can also affect adults, possibly due to repeated strain on the abdomen.
Hiatus hernias
Unlike the inguinal hernias, hiatus hernias have nothing to do with the abdominal wall and occur in the chest area and affect the digestive system.
The esophagus (food pipe that connects your throat and stomach) goes through the hiatus and attaches to your stomach. Hiatus is the small opening in the diaphragm through which the esophagus passes.
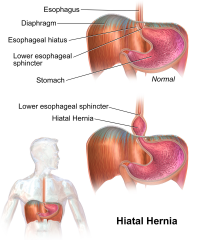
By BruceBlaus – Own work, CC BY-SA 4.0, Wikipedia Commons
This hiatus is responsible for preventing stomach contents which include acids from flowing back into the esophagus, i.e. upwards, which is called reflux.
If the area of the hiatus is weak, this function is weakened, the result being the reflux of acidic digestive juices in the stomach pushed up into the esophagus.
As a result, the lining of the esophagus which is not protected against the action of these acids is damaged leading to esophagitis.
The outcome of this is often a painful burning sensation. Other symptoms patients suffer include severe chest pain which may extend to just below the shoulder blades and heartburn.
Unlike an abdominal hernia, there is no bulge in hiatus hernia. The diagnosis is usually made by a doctor and is confirmed by X-ray and endoscopy.
What causes hiatus hernia is not clear, but it may be the result of the diaphragm becoming weak with age or due to the pressure on the abdomen.
Other types of hernia
Other types of hernia that can affect the tummy include:
- Incisional hernias – where tissue protrudes through a prior surgical/incisional wound in your abdominal wall that has not fully healed or has weakened the abdominal wall
- Epigastric hernias – where fatty tissue protrudes through your abdomen, between your belly button and the lower part of your breastbone (linea alba.)
- Spigelian hernias – where part of your bowel protrudes through your tummy at the side of your abdominal muscle, below your belly button
- Diaphragmatic hernias – where organs in your abdomen move into your chest through an opening in the diaphragm ( the dome-shaped muscle between the chest and abdomen that helps you breathe). This can also affect babies if their diaphragm does not develop properly in the womb. When present this can be a medical emergency.
- Muscle hernias – where part of a muscle protrudes through your abdomen; they also occur in leg muscles as the result of a sports injury.
A brief history of Hernia treatment
Although Hernia was present in human history from its very beginning it was first diagnosed by the Egyptians (1500BC) the Phoenicians ( 900 BC) and the ancient Greeks (Hippocrates, 400 BC).
According to the Egyptian Papirus of Ebers hernia is swelling that comes out during coughing.
Surgical and non-surgical treatments existed and surgery was used as a last resort in critical cases.
Clear evidence of this is the complete absence of the scrotum in the mummy of the Pharaoh Merneptah (1215 BC) and a hernial sac (in the groin) in the mummy of Ramses V (1157 BC).
One method involved the pressure of a finger or hand to reduce the displaced organ or tissue and then maintaining the herniated content by using a belt or girdle as support.
Belts were popular as other options for treatment were considered dangerous.
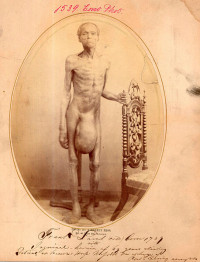
A man with a 69 years history of inguinal hernia. From: Otis Historical Archives of “National Museum of Health and Medicine”.
An early attempt to solve inguinal hernia by using a surgical knife came from the famous 26th-century Italian anatomist, Gabriele Fallopio.
Fallopio proposed wide excision of the sac with surrounding skin and all its contents, securing the neck with an impressive suture.
The technique soon turned out to be unpopular as it resulted in castration and risk of death from bleeding.
In the late 1900s after the introduction of antisepsis, asepsis, and anesthesia, Eduardo Bassini in 1887, demonstrated the first true hernia repair using advanced surgical techniques.
EDOARDO BASSINI
Bassini, in 1884, devised a method of hernia repair that called for a three-layer reconstruction of the inguinal floor.
It was Bassini who came up with the idea that only complete reconstruction of the anatomy of the inguinal canal can lead to a full recovery from inguinal hernia.
Between 1883 to 1889 he operated on 274 hernias.
Probably the last big step in the evolution of the “tension” repairs of inguinal hernias was the method described and mastered over the years by Edward Earl Shouldice from Toronto.
In 1935 Wallace Carothers, a chemist at Dupont, discovered a method to create synthetic polymers and is credited with the creation of Nylon.
The “era of plastics” was ushered in and other polymers like polyester and polypropylene were discovered and used in the manufacture of countless items including surgical mesh.
Starting in the 1940s various forms of synthetic polymers were used in inguinal hernia repair. By the 1960s, Dr. Richard Newman had performed over 1600 inguinal hernia repairs using polypropylene.
It was Irvin Lichtenstein from Los Angeles who in 1984 proposed repairing the posterior wall of the inguinal canal with mesh without previous incision and reconstruction.
Lichtenstein tension-free hernia repair is still one of the most commonly performed procedures in the world and is considered the gold standard in the united states due to the low complication rate.
The first laparoscopic inguinal hernia surgery was first performed in 1979 by P. Fletcher but, it wasn’t until 1989 that a prosthetic mesh was used during laparoscopic hernia repair.
Over the next decade, various laparoscopic methods like (transabdominal preperitoneal) TAPP and (totally intraperitoneal) TEP were introduced.
Resources: NHS website History of the Inguinal Hernia Repair
The author acknowledges the use of authentic medical literature from reputed media to structure this article.
The contents of this article are not meant to be a substitute for medical advice, diagnosis, or treatment, and should not be construed or treated as such. Always seek the advice of your physician or another qualified health provider with any questions you may have regarding a medical condition. We make no representations, warranties, or guarantees, whether express or implied, that the content on our website is accurate, complete, or up to date.
Sign up for the QuackTrack.org newsletter below!